JANUARY 23, 2014 BY CHIROTRUST
The Potential Viability of Omega-3 Essential Fatty Acids as an Anti-Inflammatory Agent
We are going to deviate from the mechanical discussions of joint pain treatment. Usual topics such as physiotherapy, stretching, manipulation, etc… and instead we’re going to discuss what looks to be aremarkably inexpensive yet potentially valuable tool in combating joint pain and inflammation.
Far removed from today’s ultra-popular yet often little tested “health foods” and “supplements” this tool has undergone testing and research typically avoided by “natural substances” and we’ll be discussing those studies in just a little bit.
The tool I’m referring to is the“Omega-3 Essential Fatty Acids”
Fatty acids are a chain (of variable length) of carbon atoms that have a starting carboxyl group (-COOH). The ending carbon of the chain is known as the omega carbon. The ending omega carbon is also a methyl group, meaning it is bonded with three hydrogen atoms (-CH3).
There are four broad categories of fatty acids***:
(see the appendix of this issue for a detailed chemistry primer of fatty acids and their components)
Saturated
Monounsaturated
Omega-3 polyunsaturated
Omega-6 polyunsaturated
Importantly, both omega-6 and omega-3 fatty acids are essential for human health, and our patient’s bodies do not have the ability to create them from other fatty acids.
Consequently, both omega-6 and omega-3 fatty acids must be consumed in the diet. Dietary deficiencies in either omega-6 or omega-3 fatty acids are deleterious to our patients health.
Additionally, the ratio of omega-6 to omega-3 fatty acids is critically important. “Historical estimates place the ratio of omega-6 to omega-3 oils at nearly 1:1 for prehistoric humans.”
The ratio of omega-6 to omega-3 fatty acids has changed dramatically due to the widespread use of vegetable oils (mostly n-6 fats) in cooking and foods.
By 1900, the ratio of omega-6 to omega-3 fatty acids had increased to about 4:1.
The current American ratio is about 25:1.
This “sharp rise is due to increased vegetable oil consumption: from 2 lb. per year in 1909 to 25 lb. per year in 1985!” (Mark Boswell and B. Eliot Cole, editors;American Academy of Pain Management Weiner’s Pain Management, A Practical Guide for Clinicians; Seventh Edition, 2006, pp.584-585.)
*(For the biological enzymatic processing of omega-6 fatty acids schematic see the appendix at the end of this issue)
A critically important aspect of essential fatty acid biology is…
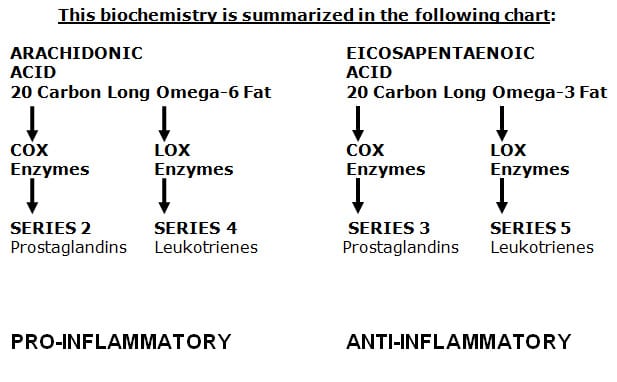
The 20-carbon long omega-6 and omega-3 fatty acids are the precursors to a group of powerful but short-lived hormone-like compounds called “eicosanoids.”
One category of eicosanoids is referred to as “prostaglandins.”
Another group is referred to as “leukotrienes.”
Clinical applications of this biochemistry includes:
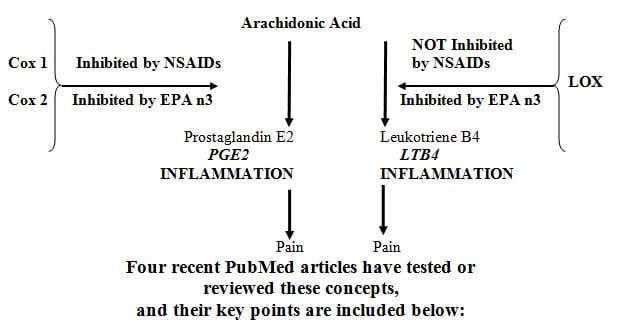
Arachidonic Acid (AA), the 20-carbon long omega-6 fatty acid is enzymatically converted into the eicosanoids called “series 2 prostaglandins,” such as “Prostaglandin E2 (PGE2),” by enzymes referred to as “cyclo-oxygenase” or “COX.”
Prostaglandin E2 is pro-inflammatory, which alters the threshold of the pain afferent neurons in the region, and patients experience increased pain.
Arachidonic Acid (AA), is also enzymatically converted into the eicosanoids called “series 4 leukotrienes,” such as “Leukotriene B4 (LTB4),” by enzymes referred to as “lipo-oxygenase” or “LOX.”
Leukotriene B4 is also pro-inflammatory, and patients experience increased pain.
Eicosapentaenoic acid (EPA), the 20-carbon long omega-3 fatty acid is enzymatically converted into the eicosanoids called “series 3 prostaglandins,” such as “Prostaglandin E3 (PGE3),” by the same cyclo-oxygenase (COX) enzymes that convert arachidonic acid into pro-inflammatory prostaglandin E2.
Historically, the conversion of arachidonic acid into pro-inflammatory prostaglandin E2 has been inhibited by utilization of nonsteroidal anti-inflammatory drugs (NSAIDs) that block the cyclo-oxygenase (COX) enzymes.
However, as noted in the article reviews below, long-term use of these drugs can cause problems in some patients.
Additionally, the article reviews below indicate that nonsteroidal anti-inflammatory drugs (NSAIDs) do not inhibit the lipo-oxygenase (LOX) pathway and therefore do not inhibit the formation of pro-inflammatory series 4 leukotrienes.
In contrast the omega-3 fatty acidEicosapentaenoic acid (EPA) inhibits both cyclo-oxygenase (COX) and lipo-oxygenase (LOX) enzymes, reducing the production of both pro-inflammatory prostaglandin E2 and series 4 leukotrienes.
Pain:
“Omega-3 Fatty acids (fish oil) as an anti-inflammatory: an alternative to nonsteroidal anti-inflammatory drugs for discogenic pain”
Surgical Neurology 65 (April 2006) 326– 331 This paper won first prizein the poster competition at the American Association of Neurological Surgeons Annual Meeting, New Orleans, LA, April 2005
Joseph Charles Maroon, MD, Jeffrey W. Bost, PAC
These authors are from the
Department of Neurological Surgery, University of Pittsburgh Medical Center
FROM ABSTRACT:
Background:
The use of NSAID medications is a well-established effective therapy for both acute and chronic nonspecific neck and back pain.
Extreme complications, including gastric ulcers, bleeding, myocardial infarction, and even deaths, are associated with their use.
An alternative treatment with fewer side effects that also reduces the inflammatory response and thereby reduces pain is believed to be omega-3 EFAs found in fish oil.
We report our experience in a neurosurgical practice using fish oil supplements for pain relief.
Methods:
From March to June 2004, 250 patients who had been seen by a neurosurgeon and were found to have nonsurgical neck or back pain were asked to take a total of 1200 mg per day of omega-3 EFAs (eicosapentaenoic acid and decosahexaenoic acid) found in fish oil supplements.
Results:
78% were taking 1200 mg and 22% were taking 2400 mg of EFAs.
After an average of 75 days on fish oil:
59% discontinued to take their prescription NSAID medications for pain.
88% stated they were satisfied with their improvement and stated they would continue to take the fish oil.
There were no significant side effects reported.
Conclusions:
Our results mirror other controlled studies that compared ibuprofen and omega-3 EFAs demonstrating equivalent effects in reducing arthritic pain.
Omega-3 EFA fish oil supplements appear to be a safer alternative to NSAIDs for treatment of nonsurgical neck or back pain.
KEY POINTS FROM AUTHORS
Maroon & Bost from
Department of Neurological Surgery,
University of Pittsburgh Medical Center
1) The use of NSAIDs is associated with occasional extreme complications, including gastric ulcers, bleeding, myocardial infarction, stroke, and even death.
2) In this study, after 75 days on fish oil, 59% of patients who were taking NSAIDs for chronic spinal pain and who had degenerative spine disease, were able to discontinue their prescription NSAIDs, and 88% stated they were satisfied with their improvement and that they would continue to take the fish oil.
3) In this study, fish oil supplementation was not associated with any significant side effects.
4) “Omega-3 EFA fish oil supplements appear to be a safer alternative to NSAIDs for treatment of nonsurgical neck or back pain.”
5) “More than 70 million NSAID prescriptions are written each year, and 30 billion over-the-counter NSAID tablets are sold annually.”
6) “5% to 10% of the adult US population and approximately 14% of the elderly routinely use NSAIDs for pain control.”
7) Selling NSAIDs is a 9 billion dollar per year US industry.
8) Prescription NSAIDs for rheumatoid and osteoarthritis alone conservatively cause 16,500 deaths per year.
9) “NSAIDs are the most common cause of drug-related morbidity and mortality reported to the FDA and other regulatory agencies around the world.”
10) “The agent best documented by hundreds of references in the literature for its anti-inflammatory effects is omega-3 EFAs found in fish and in pharmaceutical-grade fish oil supplements.”
11) The beneficial anti-inflammatory affects of high-dose fish oil include the reduction of joint pain from rheumatoid and osteoarthritis, improvement in dry eyes and macular degeneration, reduced plaque formation, reduced arrhythmias, and reduced infarction from coronary arthrosclerosis.
12) COX-2 inhibitors significantly increase gastric and cardiovascular side effects.
13) Omega-3 EPA is used to make the anti-inflammatory eicosanoids (PGE3), whereas excess omega-6 EFAs form inflammatory arachidonic acid based eicosanoids (PGE2).
14) “Animal proteins, especially red meat, also contain an abundant amount of arachidonic acid.”
15) A deficiency in omega-3 fatty acids, especially EPA, will result in a deficiency of anti-inflammatory prostaglandins.
16) “To encourage the production of anti-inflammatory PGs and to discourage the production of inflammatory PGs, saturated fats, trans-fatty acids, and arachidonic acid should be reduced in the diet; blood glucose should be controlled; and appropriate amounts of omega-3 fatty acids found in fish oils should be consumed.”
17) Omega-3 supplementation is safe and effective for many inflammation-related conditions and has a low incidence of side effects.
18) “The US Department of Agriculture has limited fish consumption to 1 fish serving per week in adults and even less in children and pregnant women because of the concern of toxic contaminants such as mercury, polychlorinated biphenyls, and dioxin in our fish population.”
19) These authors did not recommend the fish oil for those on anticoagulants or fish-related allergies, but noted “aspirin use was not a contraindication.”
Fish oil:
what the prescriber needs to knowArthritis Research & Therapy Volume 8, Issue 1, 2006, pp. 402
Leslie G Cleland, Michael J James and Susanna M Proudman
FROM ABSTRACT:
There is a general belief among doctors, that patients with arthritis need nonsteroidal anti-inflammatory drugs (NSAIDs).
Implicit in this view is that these patients require the symptomatic relief provided by inhibiting synthesis of nociceptive prostaglandin E2, a downstream product of the enzyme cyclo-oxygenase (COX), which is inhibited by NSAIDs.
However, the concept of ‘safe’ NSAIDs has collapsed following a multiplicity of observations establishing increased risk for cardiovascular events associated with NSAID use, especially but not uniquely with the new COX-2-selective NSAIDs. This mandates greater parsimony in the use of these agents.
Fish oils contain a natural inhibitor of COX, reduce reliance on NSAIDs, and reduce cardiovascular risk through multiple mechanisms.
Fish oil thus warrants consideration as a component of therapy for arthritis, especially rheumatoid arthritis, in which its symptomatic benefits are well established.
A major barrier to the therapeutic use of fish oil in inflammatory diseases is ignorance of its mechanism, range of beneficial effects, safety profile, availability of suitable products, effective dose, latency of effects and instructions for administration. This review provides an evidence-based resource for doctors and patients who may choose to prescribe or take fish oil.
KEY POINTS FROM AUTHORS
Cleland, James & Proudman as Published in
Arthritis Research & Therapy
1) There is a general belief among doctors that patients with arthritis need nonsteroidal anti-inflammatory drugs (NSAIDs). This is because the pain of arthritis is primarily caused by PGE2, which is derived from the omega-6 fatty acid arachidonic acid through the activity of the enzyme COX. NSAIDs inhibit the COX enzyme.
2) However, NSAIDs increase the risk for cardiovascular events.
3) Fish oils contain a natural inhibitor of COX, reduce reliance on NSAIDs, and reduce cardiovascular risk.
4) Omega-6s (n6) and omega-3s (n3) are dietary essential fatty acids which cannot be synthesized endogenously.
5) Diets in industrialized Western countries are generally abundant in n6 PUFAs and poor in n3 PUFAs.
6) “Because Western diets are typically low in LC n3 PUFAs, substantial increases in tissue LC n3 can be achieved by taking a fish oil supplement.”
7) It is unlikely that one can consume the amount of fish required to achieve anti-inflammatory doses (minimum of 2.7 g/day) of LC n3 PUFAs.
8) “The conversion of C18 n3 PUFAs [such as flax oil] to C20 and C22 n3 PUFAs [fish oil] occurs relatively inefficiently in humans, and so vegetable sources of dietary n3 PUFAs alone fail to achieve the tissue levels seen with fish oil.”
9) “EPA [fish oil omega-3] is both an inhibitor of arachidonic acid metabolism and an alternate substrate for COX.”
10) “EPA [fish oil omega-3] also inhibits the metabolism of arachidonic acid into leukotriene B4 by LOX enzymes, which NSAIDs do not do. Consequently, EPA fish oil is superior to NSAIDs in creating an anti-inflammatory effect.”
11) “The anti-inflammatory dose of fish oil requires delivery of 2.7 g or more of long chain n3 PUFAs daily.”[Important]
12) A daily intake of less than 2.7 g eicosapentaenoic acid (EPA) plus docosahexaenoic acid (DHA) is “insufficient for an anti-inflammatory effect.”
13) Symptomatic improvement from fish oil supplementation can take 2–3 months, and “it is important that potential users understand that this delay exists.”
14) Patients should also reduce ingestion of n6 PUFA by substituting olive oil for vegetable oils.
15) “At anti-inflammatory doses, cod liver oils, which are rich in the fat-soluble vitamins A and D, contain more vitamin A than recommended intakes.” Vitamin A has been associated with reduced bone density and increased risk for hip fracture.
16) Vitamin A toxicity is not a problem with anti-inflammatory doses of fish body oils because they contain very little vitamin A.
17) “Fish oil (obtained from the body of the fish) is preferable to cod liver oil, which can deliver undesirable amounts of vitamin A at anti-inflammatory doses.”
18) “Within the Western context, fish oil supplements have not been associated with an increased bleeding tendency, even in patients taking aspirin or warfarin for antithrombotic effect.”
19) “Methylmercury is an industrial contaminant that accumulates in long-lived fish (e.g. swordfish, marlin, sea perch, shark).”
20) “Methylmercury is a neurotoxin that impairs neural development, especially in the foetus and infants.”
21) Fish consumption is associated with increased blood and urine mercury.
22) “Properly processed fish oils contain very little mercury.”
23) “Chlorinated biphenyls (PCBs) are byproducts of industrial synthesis of organic chemicals. They are structurally related to dioxins and are potentially toxic.”
24) PCBs are poorly biodegradable and they accumulate in the land and marine food chains.
25) Polybrominated biphenyl (PBB) fire retardants are similar to PCBs.
26) “Halogenated biphenyls can be removed from fish oils by molecular distillation and should be present at low levels in good quality products.”
27) “In a medical environment in which messages molded by pharmaceutical interests stress the ‘need’ for NSAIDs, prescribers should consider the NSAID-sparing effects, the lack of serious side effects and the positive health benefits of fish oil.”
“A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain” Pain… May 2007, 129(1-2), pp. 210-223
Robert J. Goldberg and Joel Katz
Abbreviations:
ALA Alpha-linolenic acid
18 carbon long omega-3 plant fatty acid
EPA Eicosapentaenoic acid
20 carbon long omega-3 fish fatty acid
DHA Docosahexaenoic acid
22 carbon long omega-3 fish fatty acid
LA Linoleic acid
18 carbon long omega-6 plant fatty acid
AA Arachidonic acid
20 carbon long omega-6 animal fatty acid
FROM ABSTRACT
Between 40% and 60% of Americans use complementary and alternative medicine to manage medical conditions, prevent disease, and promote health and well-being.
Omega-3 polyunsaturated fatty acids (n-3 PUFAs) have been used to treat joint pain associated with several inflammatory conditions.
We conducted a meta-analysis of 17 randomized, controlled trials assessing the pain relieving effects of n-3 PUFAs in patients with rheumatoid arthritis or joint pain secondary to inflammatory bowel disease and dysmenorrhea.
Supplementation with n-3 PUFAs for 3–4 months reduces patient reported joint pain intensity, minutes of morning stiffness, number of painful and/or tender joints, and NSAID consumption.
The results suggest that n-3 PUFAs are an attractive adjunctive treatment for joint pain associated with rheumatoid arthritis, inflammatory bowel disease, and dysmenorrhea.
KEY POINTS FROM AUTHORS
Goldberg & Katz as Published in Pain
1) “Between 40% and 60% of Americans use complementary and alternative medicine to manage medical conditions, prevent disease, and promote health and well-being.”
2) 33% of those who use complementary medicine cite pain as the primary reason.
3) “Supplementation with n-3 PUFAs for 3–4 months reduces patient reported joint pain intensity, minutes of morning stiffness, number of painful and/or tender joints, and NSAID consumption.”
4) Omega-3 PUFAs are an adjunctive treatment for joint pain associated with rheumatoid arthritis, inflammatory bowel disease, and dysmenorrhea.
5) Nonsteroidal anti-inflammatory drugs are associated with gastrointestinal bleeding and myocardial infarction.
6) “The typical North American diet is very low in EPA and DHA and conversion is limited from dietary alpha-linolenic acid, found in vegetable oils, to EPA and DHA.”
7) Fish oil is a rich source of long-chain n-3 PUFAs EPA and DHA.
8) “In humans, supplementation with fish oil, or EPA/DHA capsules, increases the incorporation of n-3 PUFAs into phospholipids, conferring anti-inflammatory effects.”
9) The therapeutic effects of n-3 PUFAs usually manifest after approximately 3 months, and “taking n-3 PUFA supplementation for 2 months or less would not benefit significantly.” [Important]
10) Studies that provided high-dose (more than 2.7 g/day of EPA and DHA) n-3 PUFAs showed greater improvements in morning stiffness and number of painful and/or tender joints compared to low-dose n-3 PUFAs.
11) “The results of the present meta-analysis support the hypothesis that n-3 PUFA supplementation improves pain outcomes after three months, particularly with respect to patient assessed pain, duration of morning stiffness, number of painful and/or tender joints, and [reduced] NSAID consumption.”
12) “A minimum of three months of supplementation with a dose of 2.7 g/day of EPA and DHA is required to achieve an anti-inflammatory and a therapeutic effect.” [Important]
13) “Significant improvements were noted in patient assessed pain and morning stiffness among studies providing high-dose but not low-dose n-3 PUFA supplementation.”[Important]
14) “Reducing the intake of n-6 fatty acids (e.g., linoleic acid), which are metabolized to arachidonic acid and inflammatory eicosanoids, would be expected to increase the effectiveness of n-3 PUFA supplements.”
15) EPA/DHA supplements may also be useful for other types of chronic inflammatory pain, such as osteoarthritis or chronic back pain.
16) Alpha-linolenic acid [flax seed oil, etc.] is poorly converted to EPA and DHA.
17) This meta-analysis indicates that n-3 PUFA supplementation in patients with rheumatoid arthritis or joint pain secondary to inflammatory bowel disease and dysmenorrhea, reduces patient assessed joint pain intensity, morning stiffness, number of painful and/or tender joints, and reduces NSAID consumption.
Omega-3 Fatty Acids and Athletics
Current Sports Medicine Reports July 2007, 6:230–236
Artemis P. Simopoulos, MD
The Center for Genetics, Nutrition and Health, Washington, DC, USA
FROM ABSTRACT
Human beings evolved consuming a diet that contained about equal amounts of n-6 and n-3 essential fatty acids.
Today, in Western diets, the ratio of n-6 to n-3 fatty acids ranges from approximately 10:1 to 20:1 instead of the traditional range of 1:1 to 2:1.
Studies indicate that a high intake of n-6 fatty acids shifts the physiologic state to one that is prothrombotic and proaggregatory, characterized by increases in blood viscosity, vasospasm, and vasoconstriction, and decreases in bleeding time.
N-3 fatty acids, however, have anti-inflammatory, antithrombotic, antiarrhythmic, hypolipidemic, and vasodilatory properties.
Excessive radical formation and trauma during high-intensity exercise leads to an inflammatory state that is made worse by the increased amount of n-6 fatty acids in Western diets, although this can be counteracted by eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA).
For the majority of athletes, especially those at the leisure level, general guidelines should include EPA and DHA of about 1 to 2 g/d at a ratio of EPA:DHA of 2:1.
KEY POINTS FROM AUTHOR
Simopoulos
from The Center for Genetics,
Nutrition and Health, Washington, DC, USA
1) The human diet has had major changes in the past 150 years, yet the genetic profile has changed very little, if any, in the past 10,000 to 15,000 years.
2) Human beings evolved consuming a diet that contained about equal amounts of n-6 and n-3 essential fatty acids.
3) Today, in Western diets, the ratio of n-6 to n-3 fatty acids ranges from approximately 10:1 to 20:1 instead of the traditional range of 1:1 to 2:1.
4) Excessive free radical formation and trauma during high-intensity exercise leads to an inflammatory state that is made worse by the increased amount of n-6 fatty acids in Western diets, although this can be counteracted by the n-3 fish oils eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA).
5) Most athletes should include 1 to 2 g/d EPA / DHA fish oil.
6) The ratio of EPA:DHA should be 2:1.
7) Ingestion of EPA and DHA from fish or fish oil leads to:
A)) Decreased production of prostaglandin E2
B)) Decreased formation of leukotriene B4, an inducer of inflammation
8) The increased amounts of n-6 fatty acids in the Western diet increase the eicosanoid metabolic products from arachidonic acid, specifically prostaglandins and leukotrienes. Eicosapentaenoic fish oil is the primary inhibitor of this arachidonic cascade.
9) “N-3 fatty acids are essential for overall health of the athlete.”
10) Fish oil concentrates rich in EPA and DHA counteract the effects of the inflammatory state.
11) “The background diet should be balanced in n-6 and n-3 fatty acids by lowering n-6–rich oils such as corn oil, sunflower, safflower, cottonseed, and soybean oils.”
12) “Changes and improvements in the background diet and an additional 1 to 2 g/d of EPA and DHA should prevent the inflammation in muscles and joints. For the elite athlete, the above prophylactic measures are essential.”
13) “Essential fatty acids, both n-6 and n-3, have been part of our diet since the beginning of human life. Before the agricultural revolution 10,000 years ago, humans consumed about equal amounts of both. Over the past 150 years this balance has been upset.”
14) “Eicosanoids derived from n-6 fatty acids have opposing metabolic properties to those derived from n-3 fatty acids. A balanced intake of both n-6 and n-3 fatty acids is essential for health.”
A central theme in these articles is that for pain control, eicosapentaenoic acid (EPA) omega-3 is the most powerfully anti-inflammatory and pain suppressing fatty acid.
Dr. Artemis P. Simopoulos, MD, (above) from the Center for Genetics, Nutrition and Health, in Washington, DC, advocates a ratio of eicosapentaenoic acid (EPA) / docosahexaenoic acid of 2/1.
This same ratio is advocated by biochemist Barry Sears, Ph.D in his two books (The Omega Zone, Regan Books, 2002; The Anti-Inflammation Zone, ReganBooks, 2005) and by Harvard Psychiatry Professor Andrew Stoll, MD, in his book (Omega-3 Connection, Simon & Schuster, 2001).
Fish oil supplements should be of high quality (purified, pharmaceutical grade, molecular distilled) to remove contaminants that bio-accumulate in fish.
In addition to fish oil omega-3 supplementation, patients should reduce their consumption of omega-6 fatty acids in their diet.
APPENDIX – Fatty Acid Components…
Saturated fatty acids means that each carbon atom is saturated with hydrogen molecules, which means there are no carbon-to-carbon (-C=C-) double bonds.
Unsaturated fatty acid means that there are one or more carbon-to-carbon double bonds. Each carbon-to-carbon double bond necessitates the removal of two hydrogen atoms. Therefore the fatty acid molecule is referred to as being “unsaturated” with hydrogen atoms.
An example of a saturated fatty acid is stearic acid. It is 18 carbons long and has no double bonds, and therefore is considered to be “saturated” with hydrogen atoms.
C-C-C-C-C-C-C-C-C-C-C-C-C-C-C-C-C-COOH
Its chemical formula is 18:0.
The 18 means it is 18 carbons long. The 0 means there are no double bonds.
An example of a monosaturated fatty acid is oleic acid, the primary fatty acid found in olive oil. It is also 18 carbons long and has one double bond, making it “monounsaturated.”
C-C-C-C-C-C-C-C-C=C-C-C-C-C-C-C-C-COOH
Its chemical formula is 18:1n-9.
Again the 18 means it is 18 carbons long. The 1 means it has 1 double bond. The n-9 is pronounced “omega-9″ and means that the first double bond is located at the ninth carbon from the end methyl group.
Even though stearic acid and oleic acid are both 18 carbons in length, stearic acid is a solid at room temperature while oleic acid is a liquid (i.e. olive oil). This is because the more double bonds a fatty acid has, the more “fluid” it is. The addition of the single double bond at the ninth carbon is sufficient to change the fatty acid from a solid to a liquid.
Linoleic acid is an 18 carbon long omega-6 fatty acid. It is the primary fatty acid found in corn oil, cottonseed oil, safflower oil, sunflower oil, peanut oil, and in soybean oil.
C-C-C-C-C-C=C-C-C=C-C-C-C-C-C-C-C-COOH
Its chemical formula is 18:2n-6.
Once again, the 18 means it is 18 carbons long. The 2 means it has 2 double bonds. The n-6 is pronounced “omega-6″ and means that the first double bond is located at the sixth carbon from the end methyl group.
Alpha-linolenic acid is an 18 carbon long omega-3 fatty acid. It is the primary fatty acid found in flaxseed oil.
C-C-C=C-C-C=C-C-C=C-C-C-C-C-C-C-C-COOH
Its chemical formula is 18:3n-3.
Once again, the 18 means it is 18 carbons long. The 3 means it has 3 double bonds. The n-3 is pronounced “omega-3″ and means that the first double bond is located at the third carbon from the end methyl group.
Biological Enzymatic Processing Of Omega-6 Fatty Acids
Eighteen carbon long omega-6 and omega-3 fatty acids can be enzymatically converted into longer fatty acids with more double bonds. The enzymes that do this are called “elongase” and “desaturase.” This biological enzymatic processing of omega-6 fatty acids basically follows this scheme:
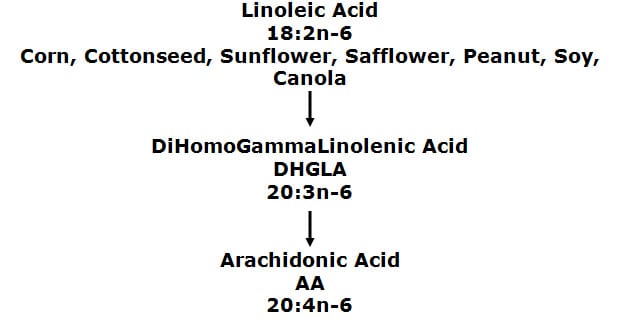
DiHomoGammaLinolenic acid (DHGLA) is a 20-carbon long omega-6 fatty acid.
C-C-C-C-C-C=C-C-C=C-C-C=C-C-C-C-C-C-C-COOH
Its chemical formula is 20:3n-6.
The 20 means it is 20 carbons long. The 3 means it has 3 double bonds. The n-6 is pronounced “omega-6″ and means that the first double bond is located at the sixth carbon from the end methyl group.
Arachidonic Acid (AA) is a 20-carbon long omega-6 fatty acid. It is the primary fatty acid found in consumable domesticated meat (beef, pork, chicken, turkey, etc.) and eggs.
C-C-C-C-C-C=C-C-C=C-C-C=C-C-C=C-C-C-C-COOH
Its chemical formula is 20:4n-6.
The 20 means it is 20 carbons long. The 4 means it has 4 double bonds. The n-6 is pronounced “omega-6″ and means that the first double bond is located at the sixth carbon from the end methyl group.
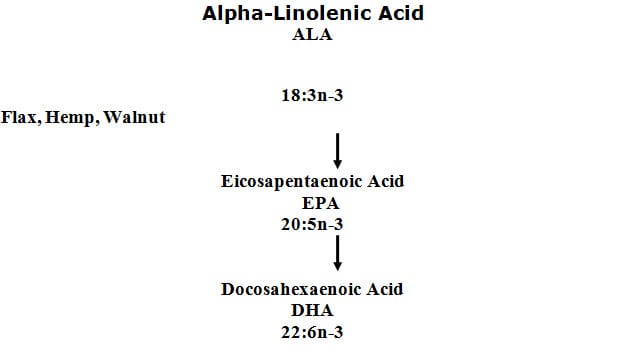
Eicosapentaenoic acid (EPA) is a 20-carbon long omega-3 fatty acid. It is the primary fatty acid found in fish oil.
C-C-C=C-C-C=C-C-C=C-C-C=C-C-C=C-C-C-C-COOH
Its chemical formula is 20:5n-3.
The 20 means it is 20 carbons long. The 5 means it has 5 double bonds. The n-3 is pronounced “omega-3″ and means that the first double bond is located at the third carbon from the end methyl group.
Docosahexaenoic acid (DHA) is a 22-carbon long omega-3 fatty acid. It is also primarily found in fish oil, yet there are algae sources as well.
C-C-C=C-C-C=C-C-C=C-C-C=C-C-C=C-C-C=C-C-C-COOH
Its chemical formula is 22:6n-3.
The 22 means it is 22 carbons long. The 6 means it has 6 double bonds. The n-3 is pronounced “omega-3″ and again means that the first double bond is located at the third carbon from the end methyl group.