DECEMBER 5, 2014 BY CHIROTRUST
Introduction
A pioneering study was published inThe New England Journal of Medicinein 1994 (1). Researchers from Hoag Memorial Hospital in Newport Beach, California, performed magnetic resonance imaging (MRI) examinations on 98 people who did not have back pain. Sixty-four percent of the 98 asymptomatic subjects were found to have abnormal lumber spine discs. The pathologies included bulging, protrusions, an extrusion and other annular defects (disruption of the outer fibrous ring of the disk); all secondary to disc degenerative disease. The age of the afflicted subjects was from 20 to 80 years (mean age, 42.3 years), and the pathologies increased with age. The authors concluded:
“These findings support the contentions that annular defects are generally associated with disk degeneration and that such defects are frequently asymptomatic.”
This study indicates that the majority of chiropractic patients, including patients who do not have back pain, have abnormalities of the intervertebral disc. Chiropractors are routinely adjusting the low backs of patients who have intervertebral disc pathology.
Anatomy
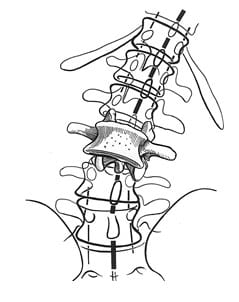
The spinal column is made up of 24 segments (vertebrae). The low back (lumbar spine) is made up of 5 segments (L1, L2, L3, L4, L5). Total spinal column motion is dependent upon the additive motion between the individual segments. Individual segmental motion is largely dependent upon the integrity of the intervertebral disc. Picture from Kapandji (2):
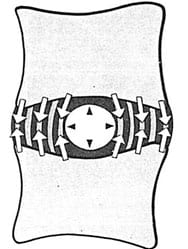
The unique anatomy of the intervertebral disc allows for both cushioning (like a shock absorber) and motion. The disc has two distinct regions:
• The nucleus pulposus:
The nucleus is mostly water and functions as a ball bearing.
• The annulus fibrosis:
The annulus is composed of tough protein fibers and cells.
Above and below each intervertebral disc is the vertebral body. The vertebral body is quite vascular (it has a well developed blood supply). Between the disc and the vertebral body is a porous cartilaginous end plate.
The intervertebral disc has no inherent blood supply. Nutrients for the cells of the intervertebral disc must travel from the vertebral body through the porous cartilaginous end plate (see Physiology below) (from reference #2).
Physiology
The adult human has approximately 75 trillion cells (3). The health and function of each cell depends upon a steady supply of nutrients (glucose, oxygen, vitamins, minerals, amino acids, etc.). For most of the cells of the human body, the delivery of these nutrients is via the blood supply. The blood is pumped to the cells by the heart, beginning with the larger arteries and eventually to the minute capillaries. The capillaries are adjacent to most of the cells of the body.
Unfortunately, the intervertebral disc is void of both arteries and capillaries. This makes the cells of the disc vulnerable to dysfunction, disease, and death. This lack of inherent vascular nutrition is the reason the intervertebral disc has increased risk for disease and degeneration (disc degenerative disease); it is also why disc injuries are notoriously slow to recover and heal.
So how do the cells of the intervertebral disc obtain the nutrients required to maintain health and function?
The answer is through motion. Anything that impairs the movement of the vertebral motor unit (two adjacent vertebrae with an intervertebral disc in between), impairs the supply of nutrients to the avascular disc.
As Vert Mooney, MD, noted in his Presidential Address to the International Society for the Study of the Lumbar Spine (4):
“Mechanical activity has a great deal to do with the exchange of water and oxygen concentration” in the disc.
An important aspect of disc nutrition and health is the mechanical aspects of the disc related to the fluid mechanics. The pumping action maintains the nutrition and biomechanical function of the intervertebral disc.
Thus, “research substantiates the view that unchanging posture, as a result of constant pressure such as standing, sitting or lying, leads to an interruption of pressure-dependent transfer of liquid. Actually the human intervertebral disc lives because of movement.”
Pathophysiology
Aging is a multifactorial phenomenon involving many variables, including time, genetics, injuries, chronic stress, nutrition, habits, etc. The aging of joints is classically called arthritis orosteoarthritis or degenerative joint disease. Degenerative joint disease of the joints of our spinal column is known as spondylosis orspondyloarthritis. The aging of the intervertebral disc is classically called degenerative disc disease.
In 2006, Susan Garstag, MD, and Todd Stitik, MD, wrote an informative article on joint degeneration (5). They attribute joint degeneration (osteoarthritis) to a number of factors, categorizing their list to local factors and systemic factors:
Local Factors include:
- Altered joint biomechanics
- Malalignment
- Muscle weakness
- Impaired proprioception neurology
Systemic Factors include:
- Age
- Genetic Factors
- Nutritional Factors, especially inflammatory profile and free radical burden (generators of oxidative stress)
Drs. Garstag’s and Stitik’s comments linking osteoarthritis to malalignment, muscle weakness, impaired proprioception, and altered joint biomechanics is particularly interesting to chiropractors, as these are all components of what chiropractors call the subluxation. Traditional chiropractic teaches that untreated joint subluxations lead to osteoarthritic changes.
Recent concepts pertaining to aging in general indicate that the aging of all of our cells is the life-long process of glycation (also known asglycosylation). This concept is nicely described by Nora Gedgaudas in 2011 (6):
“Aging is now being understood by people researching longevity as essentially a gradual process of glycation of all tissues, including the brain.” p. 126
Technically, glycation is the abnormal attachment of sugars to proteins. When a sugar attaches to a protein, the function of the protein is altered. As noted above, the proteins of the intervertebral disc are suppose to allow for the necessary motion to pump the nutritious fluids from the vertebral bodies through the cartilaginous end plates into the avascular disc. When the disc proteins are glycated with sugars, the disc becomes stiff, reducing movement, and impairing the pumping of fluid into the disc. The consequence is that the disc becomes dry (desiccated), sick, and degenerated (degenerative disc disease). This process of intervertebral disc glycation was nicely documented in an article published earlier this year by Michael Adams and colleagues from the University of Bristol, UK (7).
This process of glycation is directly linked to one’s consumption of sugars, especially fructose (6). Sadly, sugar consumption is addicting, and food scientists both know this and exploit it (8, 9). As a result, sugar has become the most successful food additive in human history. When sugar is added to food or drink, net sales (and profits) increase. If sugar is removed, sales decline. Consequently, essentially everything possible now contains added sugar (10). Sadly, this trend increases both glycation and cellular aging, including that of the intervertebral disc (6, 7).
When the proteins of the intervertebral disc become glycated, the disc itself becomes stiffer. This increased stiffness reduces motion, impairing the pumping of nutritious fluid to the cells of the disc, contributing to disc degenerative disease (8).
Another problem with glycation, is that glycated proteins increase the production of free radicals by a factor of about 50X. This is relevant in light of the osteoarthritis factors described by Drs. Garstag and Stitik above. Recall, a driving factor of osteoarthritis is one’s free radical burden and production of oxidative stress. Glycated intervertebral disc proteins and their substantially increased production of free radicals accelerate disc degenerative disease (7).
Thus, glycated disc proteins drive disc degeneration through two mechanisms, both of which were described by Drs. Garstag and Stitik above (5):
- Reducing disc motion, impairing disc nutrition.
- Increase production of free radicals, accelerating oxidative stress.
As the cells of one’s disc (or any other tissue) degenerate, the aging can be quantified. This is done by measuring the length of thetelomeres on the end of the chromosomes of the disc cells. This process was awarded the 2009 Nobel Prize in Medicine/Physiology, and is nicely described by Michael Fossel, MD, PhD, and colleagues, in 2011 (11).
Essentially, the ends of our chromosomes have a repeating sequence of nucleotide bases that are collectively referred to as thetelomere. Each time the cell divides, the telomere shortens a little. When most of the telomere disappears, the cell dies. Consequently, telomerelength has been proposed as a marker of biological aging. As noted, this concept was awarded the 2009 Nobel Prize in Medicine/Physiology to Elizabeth Blackburn, PhD, from the University of California, San Francisco, and colleagues.
This concepts of telomere shortening is true when applied to disc degenerative disease (7). As noted by Dr. Fossell and colleagues, the main drivers of cellular aging are oxidation, inflammation, and glycation (11).
The point of this discussion, and as noted with MRIs in 1994, the majority of people, and consequently the majority of chiropractic patients, have disc degenerative disease of varying degrees.
Safety
Is it safe to manipulate a low back spinal segment if that segment has disc degenerative disease?
For six decades, studies have shown that lumbar spinal manipulation is both safe and effective in the treatment of patients with low back pain, with or without leg pain, that is secondary to pathology of the intervertebral disc (12, 13, 14, 15, 16, 17, 18). Importantly, there is primary research detailing the biomechanical reason for the safety of spinal manipulation for both normal and degenerated lumbar spine intervertebral discs, noted below. It is important to understand that “torsion” is a common component of lumbar spinal manipulation.
In 1981, MA Adams, PhD, and WC Hutton, MSc, published an important study in the journal Spine, titled (19):
The Relevance of Torsion to the Mechanical Derangement of the Lumbar Spine
In their cadaver experiments, these authors noted that the limit of spinal segmental rotation was not created by the disc, but rather by the facet joint. During rotational stress, the compression facet is the first structure to yield at the limit of torsion, and this occurs after about 1-2° of rotation. “Much greater angles are required to damage the intervertebral disc, so torsion seems unimportant in the etiology of disc degeneration and prolapse.” Important statements in this article include:
“Because of the protection offered by the compression facet, the intervertebral disc is subjected to relatively small stresses and strains in the physiologic range of torsion. By the time the facets are damaged, the disc is rotated only about one-third to one-tenth of its maximum angle and is bearing a small fraction of the torque required to rupture it.”
“Except in cases of extreme trauma and as a sequel to crushing of the apophyseal joints, axial rotation can play no major part in the mechanical derangement of the intervertebral disc in life.”
Two years later, in 1983, Adams and Hutton publish an additional cadaver studies in journal Spine, titled (20):
The Mechanical Function of the Lumbar Apophyseal Joints
Based upon their experiments, they conclude that the facet joints “prevent excessive movement from damaging the discs: the posterior annulus is protected in torsion by the facet surfaces and in flexion by the capsular ligaments.” They note that the facets only allow at most 2° of rotation, and also note that the disc will completely recover from all rotational stresses that are less then 3°. These authors state:
“In flexion, as in torsion, the apophyseal joints protect the intervertebral disc.”
“The function of the lumbar apophyseal joints is to allow limited movement between vertebrae and to protect the discs from shear forces, excessive flexion, and axial rotation.”
In another follow-up article in 1995, Adams and Dolan published a study in the journal Clinical Biomechanicstitled (21):
Recent Advances in Lumbar Spinal Mechanics and their Clinical Significance
Once again, these authors note that rotational loading of a spinal motor unit will always damage the facet joints “long before the disc.” If the facet joints are removed, rotational forces will damage the disc if subjected to rotational loads between 10-20 degrees.
These authors also note “severely degenerated discs cannot be made to prolapse, presumably because the nucleus is too fibrous to exert a hydrostatic pressure on the annulus.”
The information presented by Adams, Hutton, and Dolan, indicates that for most patients suffering from a lumbar disc disease, including intervertebral disc prolapse, manipulation of the lumbar spine is both safe and often effective. These authors also specifically applied their experiments to discs that were already degenerated. Even in the presence of disc degenerative disease, these authors were able to show that rotational and torsional spinal motions did not injure these discs. They found that even in the presence of disc degeneration that the facet joints protected the disc from injury.
Outcomes
Is the manipulation of a spinal segment with disc degenerative disease helpful to the patient with low back pain?
A preliminary review of the literature to address this question was published in 2005 in the Journal of Manipulative and Physiological Therapeutics, and titled (22):
High-velocity low-amplitude spinal manipulation for symptomatic lumbar disk disease: A systematic review of the literature
The authors of this study performed a systematic review of the literature, including the Cochrane Central Register of Controlled Trials, Medline, Cumulative Index to Nursing and Allied Health Literature, and Mantis. Sixteen studies met the inclusion criteria, representing 203 total subjects. The authors concluded:
“The reviewed evidence supports the hypothesis that high velocity low amplitude spinal manipulation may be effective in the treatment of symptomatic lumbar disc disease and does not support the hypothesis that high velocity low amplitude spinal manipulation is inherently unsafe in symptomatic lumbar disc disease cases. It appears that patients with lumbar disk pathology do undergo manipulative treatment in practice. Consequently, this should be an area of research importance.”
A more recent study looking at the benefits of spinal manipulation for subjects suffering from degenerative disc disease was recently published (September 2014). The article was published in the journal Archives of Physical Medicine and Rehabilitation, and titled (23):
Short-Term Effect of Spinal Manipulation on Pain Perception,
Spinal Mobility, and Full Height Recovery in Male Subjects With Degenerative Disk Disease: A Randomized Controlled Trial
The authors point out that lumbar intervertebral disk disease is one of the main causes for low back pain. Disk degeneration is the most common pathology in the adult spine and accounting for approximately 90% of surgery cases. Subjects with symptomatic disk disorders incur the highest health care expenditure among those with other low back pain diagnoses. In agreement with above studies, degenerative disc disease is an extremely common pathology.
Disc degeneration results in structural disruption and loss of the hydrostatic capacity of the nucleus. Thus, disc degeneration eventually ends up leading to a loss of disc height with a reduction of spinal range of motion.
The purpose of the study was to evaluate, in subjects with lumbar disc degeneration, the immediate effect of a lumbosacral high-velocity low-amplitude spinal manipulation on four established variables that assess spinal function:
A) The subjects’ height viastadiometer:
The cumulative effect of the intervertebral disc loss of fluid in response to mechanical stress may reduce the subject’s measured height, spinal shrinkage. The stadiometer measures height variations and the amount of intervertebral disc compression caused by pressure on the spinal column. The stadiometer is a noninvasive method that has proven validity and is easier to use and less costly than MRI.
B) Self perceived LBP (using a visual analog scale [VAS]):
The VAS is an effective, sensitive, and appropriate tool to measure acute and chronic pain.
C) Neural mechanosensitivity:
Neural mechanosensitivity was assessed by means of the passive straight-leg raise (SLR) test. The point of initial appearance of pain or discomfort was the test endpoint, and was measured with a goniometer. The test is considered an easy-to use tool, with a reliability of 87%.
D) Spinal mobility in flexion:
Spine mobility in flexion was measured as finger-to-floor distance (FFD). This test is considered easy to conduct and has a high degree of inter-examiner reliability (96-98%).
The study was a randomized, double-blind, controlled clinical trial that evaluated 40 men with an average age of about 40 years. All subjects had degenerative lumbar disc disease at L5-S1. Twenty of the men were randomally assigned to receive a side-posture L5-S1 manipulation. The spinal manipulation was a standard side-posture very fast thrust with a short range of motion. The other 20 men were given a single placebo intervention. The placebo maneuver (sham) was also side-posture set up but involved no manipulative thrust.
Measured Outcome Improvements in Men with Degenerative Disc Disease Following a Single Side-Posture Spinal Adjustment
(rounded)
|
Measurement |
Outcome Improvement |
|
Height (stadiometer) |
4 ± 1 mm |
|
Pain (VAS) |
Reduced by 46% |
|
Neural Tension (SLR) |
Increased by 14° ± 9° |
|
Spinal Mobility (FFD) |
Increased by 4 ± 2 cm |
Results
A) Height Change Stadiometry:
- “A significant height change was found in the TG:” (3.98 ± 1.46 mm).
- The increase in paravertebral muscle activity in chronic low back pain is associated with greater compressive loads. The impact of spinal manipulation on diminishing paravertebral hyperactivity may produce changes in stadiometry (improved height).
B) Visual Analog Scale (VAS):
“The lumbosacral spinal manipulation achieved an immediate reduction in self perceived low back pain.” Pain perception decreased by 46% in in the manipulation group in relation to baseline.
C) Neural Tension Straight Leg Raise (SLR):
The passive straight-leg raising test increased with spinal manipulation by 14° ± 9° (rounded).
D) Spinal Mobility Finger-to-Floor Distance (FFD):
Spinal mobility during the finger-to-floor distance test was increased in the manipulation group by 4 ± 2 cm (rounded). It appeared that spinal manipulation modulates the somatosensory system, which inhibits the paravertebral muscle hyperactivity and improves spine function.
The authors of this study concluded:
“Ahigh-velocity, low-amplitudespinal manipulation in the lumbosacral joint performed on men with degenerative disk disease immediately improves self-perceived pain, spinal mobility in flexion, hip flexion during the passive SLR test, and subjects’ full height.”
“A side-lying spinal manipulation technique in the lumbosacral region decreases self-perceived low back pain in the short-term and produces an immediate improvement in spinal mobility in flexion, the subject’s height, and hip flexion mobility during the passive straight-leg raising test in men with disc degeneration.”
The intragroup comparison indicated a significant improvement in all variables in the spinal manipulation group compared to the control group. “In the between-group comparison of the mean differences from pre- to post intervention, there was statistical significance for all cases.”
“Only the mechanical effect from the thrust appears to be a key element to the effectiveness of the spinal manipulation.”
“Spinal Manipulation has been demonstrated to decrease pain and improve function in symptomatic lumbar disc degeneration.”
Summary
Spinal mechanical neurophysiological function is dependent upon the integrity of the intervertebral disc. The adult intervertebral disc is avascular; adult disc health depends upon motion that pumps nutrients and fluid from the adjacent vertebral bodies through the cartilaginous end plates into the disc. Any impairment in spinal segmental motion negatively impacts disc health.
The universal mechanism of cellular aging is glycation, the process of attaching sugars to proteins. The rate of glycation is linked to sugar consumption, inflammation, and oxidative stress. When the intervertebral disc is glycated it becomes stiff, reducing motion, impairing the nutritious fluid pump, accelerating degenerative disc disease. Consequently, disc degeneration is a ubiquitous adult finding. Disc degeneration is found even in asymptomatic subjects. Disc degeneration makes such individuals more susceptible to back injury and pain, and impairs recovery rates. More that half of adults have some form of low back disc degeneration.
Spinal adjusting (manipulation) at segmental levels of disc degeneration is safe. Not only it is safe, it is beneficial. The improved neuro-biomechanics that occurs as a consequence of spinal adjusting (manipulation), increases height, improves range of motion, relieves stress in the nervous system, and significantly improves pain syndrome.
REFERENCES
- Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS; Magnetic resonance imaging of the lumbar spine in people without back pain; New England Journal of Medicine; 1994 Jul 14;331(2):69-73.
- Kapamdji IA; The Physiology of the Joints; Volume 3; The Trunk and the Vertebral Column; Churchill Livingstone; 1974.
- Guyton A; Textbook of Medical Physiology; Saunders; 1981; p. 2.
- Mooney V; Where Is the Pain Coming From?; Spine; Vol. 12; No. 8; 1987’ pp. 754-759.
- Garstang SV, Stitik TP; Osteoarthritis: Epidemiology, Risk Factors, and Pathophysiology; American Journal of Physical Medicine and Rehabilitation November 2006, Vol. 85, No. 11, pp. S2-S11.
- Gedgaudas N; Primal Body, Primal Mind: Beyond the Paleo Diet for Total Health and a Longer Life; Healing Arts Press; 2011.
- Adams MA, Lama P, Zehra U, Dolan P;Why Do Some Intervertebral Discs Degenerate, When Others (in the Same Spine) Do Not?; Clinical Anatomy; April 19, 2014 [epub].
- Kessler DA; The End of Overeating: Taking Control of the Insatiable American Appetite; Rodale; 2009.
- Moss M; Salt, Sugar, Fat: How the Food Giants Hooked Us; Random House; 2013.
- Lustig R; Fat Chance: Beating the Odds Against Sugar, Processed Food, Obesity, and Disease; Hudson Street Press; 2013.
- Fossel M, Blackburn G, Woynarowski; The Immortality Edge: Realize the Secrets of Your Telomeres for a Longer, Healthier Life; Wiley; 2011.
- Ramsey RH; Conservative Treatment of Intervertebral Disk Lesions; American Academy of Orthopedic Surgeons, Instructional Course Lectures; Volume 11, 1954, pp.118-120.
- Mathews JA and Yates DAH; Reduction of Lumbar Disc Prolapse by Manipulation; British Medical Journal September 20, 1969, No. 3, 696-697.
- Edwards BC; Low back pain and pain resulting from lumbar spine conditions: a comparison of treatment results; Australian Journal of Physiotherapy; 15:104, 1969.
- White AA, Panjabi MM; Clinical Biomechanics of the Spine; Second edition, JB Lippincott Company, 1990.
- Turek S; Orthopaedics, Principles and Their Applications; JB Lippincott Company; 1977; page 1335.
- Kuo PP and Loh ZC; Treatment of Lumbar Intervertebral Disc Protrusions by Manipulation; Clinical Orthopedics and Related Research. No. 215, February 1987, pp. 47-55.
- Cassidy JD, Thiel HW, Kirkaldy-Willis WH; Side posture manipulation for lumbar intervertebral disk herniation; Journal of Manipulative and Physiological Therapeutics; February 1993;16(2):96-103.
- Adams MA and Hutton WC, MSc; The Relevance of Torsion to the Mechanical Derangement of the Lumbar Spine; Spine; Volume 6, Number 3, May/June 1981, pp. 241-248.
- Adams MA and Hutton WC, MSc; The Mechanical Function of the Lumbar Apophyseal Joints; Spine; Volume 8, Number 3, April 1983, pp. 327-330.
- Adams MA and Dolan P; Recent advances in lumbar spinal mechanics and their clinical significance; Clinical Biomechanics; Volume 10, Number 1, 1995, pp. 3-19.
- Lisi AJ, Holmes EJ, Ammendolia C; High-velocity low-amplitude spinal manipulation for symptomatic lumbar disk disease: a systematic review of the literature; J Manipulative Physiol Ther. 2005 Jul-Aug;28(6):429-42.
- Vieira-Pellenz F, Oliva-Pascual-Vaca A, Rodriguez-Blanco C, Heredia-Rizo AM, Ricard F, Almazán-Campos G; Short-term effect of spinal manipulation on pain perception, spinal mobility, and full height recovery in male subjects with degenerative disk disease: a randomized controlled trial; Arch Phys Med Rehabil; 2014 Sep;95(9):1613-9.
“Authored by Dan Murphy, D.C.. Published by ChiroTrust™ – This publication is not meant to offer treatment advice or protocols. Cited material is not necessarily the opinion of the author or publisher.”