The Weston A. Price Foundation
Posted on April 10, 2013 by Christopher Masterjohn
In April of 2011, I posted a rebuttal of a Nature paper from Stanley Hazen’s group at the Cleveland Clinic arguing that choline from animal foods causes heart disease:
Does Dietary Choline Contribute to Heart Disease?
Their argument was that our intestinal bacterial convert choline to trimethylamine, which our livers then convert to trimethylamine oxide (TMAO), which causes atherosclerosis in mice, and thus, by extension, probably in humans. I pointed out that previous studies have shown that supplements with salts of free choline do in fact generate TMAO, but uncontaminated phosphatidylcholine, the main form of choline found in food, does not. Moreover, choline-rich foods like liver and eggs did not produce more TMAO than a control breakfast, but seafood, which is generally contaminated with some trimethylamine or TMAO, did.
In a new paper in Nature Medicine, these authors have expanded their argument to claim that the carnitine in red meat contributes to heart disease through the same pathway. Put on your seat belts, folks, and let’s take a look!
The new paper can be found here:
The press reported on the paper widely, and this New York Times article by Gina Kolata gave it a big boost in popularity:
Culprit in Heart Disease Goes Beyond Meat’s Fat
In brief, here is the “clean version” of the story. The authors showed that eating a steak increased blood and urine levels of TMAO in five omnivores, whereas the same meal did not have this effect in a vegan. Furthermore, carnitine supplements increased blood TMAO in five omnivores, but not in five vegetarians and vegans. Baseline blood levels of TMAO were also higher in 30 omnivores than in 23 vegetarians and vegans, as were the levels of certain strains of intestinal bacteria. Antibiotics suppressed TMAO levels in five omnivores, showing the role of intestinal flora in its generation. Plasma concentrations of carnitine and TMAO correlated with atherosclerosis in just under 2,600 humans, and, like they had previously shown for choline, carnitine produced atherosclerosis in female mice genetically engineered to be vulnerable to that disease, but not when the mice were kept germ-free with antibiotics.
Overall, parts of this study are very well conducted, providing insights into metabolism that should fascinate anyone who loves biochemistry for its own sake and doesn’t mind meandering down rabbit holes that have no clear relevance to the health of humans or natural strains of animals. The problems with this study and its portrayal in the media are the often-times incomplete reporting of data in the paper and the wild runaway inferences published all over the press, particularly the conclusion that red meat contributes to heart disease by generating TMAO, and the even stranger notion that we should eat less red meat for this reason. Let’s take a look at the less “clean” version of the story.
Why Single Out Red Meat?
First of all, why pick on red meat? As I pointed out in my last post on this topic, lots of foods seem to increase TMAO in humans and red meat does not stand out among them. A 1999 study in six human volunteers evaluated excretion of trimethylamine and TMAO after consumption of a handful of supplements and 46 different foods. For comparison, the new paper in Nature Medicine reported data for one food (red meat) fed to two (urine data) or six volunteers (plasma data). Consistent with a 1983 finding from the group of famed choline researcher Steven Zeisel that salts of free choline but not uncontaminated phosphatidylcholine (lecithin) generated trimethylamine, this group found that high-dose choline and carnitine, but not lecithin, generated TMAO. Eight ounces of carnitine-rich foods, however, like red meat, produced no more TMAO than common fruits and vegetables. Seafoods, by contrast, led to large increases in TMAO. Let’s take a look at some of this data.
The authors compared eight ounces of 46 foods eaten with a “light breakfast” free of seafood to the “light breakfast” alone, which acted as a control. It would appear from the data that the “light breakfast,” which the authors did not describe any further, generated some TMAO. In each graph below, an asterisk indicates a statistically significant difference between the food in question eaten with the breakfast and the control breakfast alone. Lack of statistical significance relative to the control does not mean the food did not generate any TMAO, though statistical significance makes the generation of TMAO more clear. Nevertheless, it should primarily be taken to mean that the food actually stands out relative to other foods as a source of TMAO.*
Here’s a comparison between the control, beef, and a variety of fruits and vegetables:
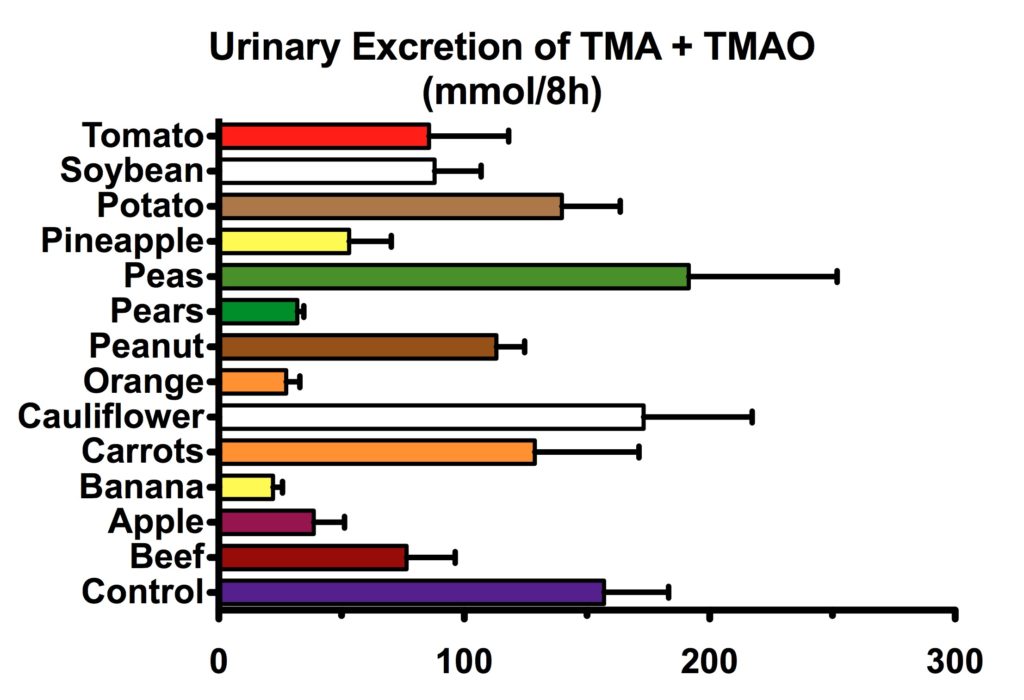
We can see that none of these foods statistically stands out from the control. Looking at the numbers alone, this “light breakfast” alone, along with carrots, cauliflower, peanuts, peas, potatoes, soybeans, and tomatoes generated more trimethylamine and TMAO than beef. In general, we could say that there is no clear evidence that beef produces more or less TMAO than any of the fruits and vegetables tested.
Here we see that none of the meats tested were statistically different from the “light breakfast” control alone (numerically, all of them except lamb liver were lower), and that there is no relation to the “redness” of the meat, with chicken having an almost identical value to beef:

Here we see that mushrooms and an assortment of grain and dairy products are statistically no different from the “light breakfast” control alone, and that bread, mushrooms, cheese and eggs all produced numerically (but not statistically) higher values than beef:

Now here’s the real kicker. What foods do stand out as supreme sources of TMAO? Seafoods! Let’s take a look at these boneless seafoods first:

Here we see that, unlike beef, all the boneless seafoods (in which I’ve included invertebrates as well as cartilaginous fish) tested except cockles produced statistically significantly more TMAO than the “light breakfast” control alone. Based on my own statistical test,** all of the seafoods shown in the graph except clams and cockles produced significantly more TMAO than beef.
Now let’s take a look at the bony fish:

All the fish except trout produced statistically more TMAO than the “light breakfast” control alone. My own statistical analysis** indicates that all the fish except tuna, trout, plaice, and the two samples of roe produced significantly more TMAO than beef.
The single “representative female omnivore” from the Nature Medicine paper excreted similar amounts of TMAO in her urine as the six subjects from the 1999 study after consuming red meat,*** suggesting that, had they measured the response to seafood, the authors of the Nature Medicine paper would also have found much greater excretion of TMAO after consumption of seafood than after consumption of red meat.
The difference between seafoods and red meat in the 1999 paper is like the difference between night and day. To take the most extreme example, halibut generated over 107 times as much TMAO as red meat. It seems obvious from this study that if any foods should be singled out for the production of TMAO, it should be seafoods. Yet the Nature Medicine paper makes no mention of fish and the New York Times article only mentions fish to point out that it has less carnitine than red meat (and thus, by inference, will generate less TMAO, though that is clearly not the case, presumably because seafood tends to be contaminated with trimethylamine or TMAO itself; see Tom’s comment).
If we are to single out red meat as a source of TMAO, we should be able to identify other foods with which it should be replaced that generate less TMAO. Yet this 1999 study, which had a small sample size but tested an expansive number of foods, found that there basically are no other foods that generate meaningfully less TMAO than red meat.
Do Meat-Eaters Generate More TMAO From Steak Than Vegans?
Do meat-eaters produce more TMAO from steak than vegans? The “clean” version of the story is, as described in the New York Times, “the answers were: yes, there was a TMAO burst in the five meat eaters; and no, the vegan did not have it.” The data presented in the Nature Medicine paper are less clear.
First, as I’ll explain in more detail below, no one ate steak alone. They ate steak with 250 milligrams of supplemental carnitine.

It certainly seems from Figure 2a, shown above, that the single “representative female omnivore” whose data is shown had a greater TMAO increase after consuming steak + carnitine than the one male vegan they were able to convince to eat the same meal. The vegan had no increase and the omnivore’s levels roughly tripled. Since the sample size is one per group, the authors did not report a statistical analysis, so we cannot make any comparison between “omnivores” as a group and “vegans” as a group.
Besides this, this same group has previously shown that the enzyme responsible for converting trimethylamine to TMAO is suppressed by androgens, and its activity is low in males compared to females. Thus, comparing a female omnivore to a male vegan is misleading.
In any case, it’s not so clear once we look at the supplementary figures, or once we read the main text, how “representative” this female omnivore actually was.
In Supplementary Figure 5, we find this schematic and data of one person’s three steak + carnitine challenges:

The legend says this is data for “a representative omnivorous subject” (they do not specify the person’s gender). Prior to antibiotic treatment, shown on the left, the TMAO remained flat over 24 hours after consuming a steak and carnitine supplement. We only see an increase after this omnivore was given antibiotics and his or her intestinal flora grew back over a week, shown on the right, and in that case it didn’t even double after the steak, let alone triple as in Figure 2a. Did this subject develop dysbiosis from the course of antibiotics, and is that why TMAO increased after antibiotics but not before antibiotics?
If, prior to antibiotics, this person’s TMAO remained flat after consuming steak + carnitine, while the TMAO of the omnivore shown in Figure 2a nearly tripled, how can they both be “representative”? Is the data in Supplementary Figure 5 from a male, and does this represent a fundamental difference between males and females? Is the data shown in Figure 2a “representative” of a female omnivore before or after she was given antibiotics? If the latter, does the increase simply represent the effects of antibiotic-induced dysbiosis?
As mentioned above and as can be seen in the top of Supplementary Figure 5, moreover, the subjects did not simply consume steak. Along with the steak, the authors fed carnitine labeled with a heavy isotope (d3), which is like a chemical tag that allowed the investigators to trace its metabolism. If they observed labeled TMAO in the blood, this would show that the carnitine was converted to TMAO. Indeed, they showed this in a single “representative female omnivorous subject” in Figure 1e. But the amount of labeled TMAO in the blood would be tiny compared to the total amount of TMAO. If we are evaluating the plausibility of the hypothesis that TMAO in the blood contributes to heart disease, we care about the total amount of TMAO. The question, then, is whether eating steak leads to a meaningful increase in total TMAO. Here is what the authors had to say:
In most subjects examined, despite clear increases in plasma d3-carnitine and d3-TMAO concentrations over time (Fig. 1e), post-prandial changes in endogenous (unlabeled) carnitine and TMAO concentrations were modest (Supplementary Fig. 5), consistent with total body pools of carnitine and TMAO that are relatively very large in relation to the amounts of carnitine ingested and TMAO produced from the carnitine challenge.
It is unclear what “modest” means in this context. Nowhere appear any data for the entire group of omnivores. We just have a “represenatative” graph in Supplementary Figure 5 where the TMAO increase is non-existent, not “modest,” prior to antibiotics, and another “representative” graph in Figure 2a where the result is very different. Since both relevant graphs have a sample size of one, there is no statistical analysis. The authors seem to be saying in the above paragraph, however, that, on the whole, the non-existent increase in total TMAO shown in Supplementary Figure 5 is more representative than the large increase shown in Figure 2a.
If the labeled TMAO increased after the steak + carnitine challenge but the total pool of TMAO did not, this indicates that carnitine was converted into TMAO, but that the TMAO generated from the carnitine was so small compared to the amount of TMAO already present in the body as to be largely irrelevant.
Finally, we should note that the steak + carnitine challenge provided 180 milligrams of carnitine from meat and 250 milligrams of isotopically labeled carnitine from a supplement. There is no data in this paper showing that TMAO increases in response to steak alone in anyone.
Does Carnitine Increase TMAO More in Meat-Eaters Than in Vegans and Vegetarians?
After these investigators gave five meat-eaters antibiotics to show that suppressing intestinal flora would suppress TMAO, they gave five vegetarians and vegans and five omnivores a labeled carnitine supplement without any steak. It is unclear whether these omnivores are the same omnivores who previously underwent three steak + carnitine challenges, involving the use of antibiotics. In one section of the methods, the omnivores who received antibiotics are described as “additional omnivores,” but in another section they seem to be described as a “subset of subjects” who participated in the carnitine alone challenge. If they are the same omnivores, then this experiment is seriously confounded since the investigators never gave any vegetarians antibiotics. In any case, here we encounter a graph that actually includes all ten subjects instead of a “representative” subject from each group:

The most impressive thing about this graph that should jump out at us is that the standard error bars for the omnivores cover almost the entire vertical axis of the graph. If you are unfamiliar with statistics and wish to get a sense of how dramatic this degree of variation is, one way would be to scroll up to the data I showed for the 1999 study measuring TMAO generation from 46 different foods, where the bars represent the same measure of variation. The variation in that study was quite large for many foods, but not like this. For all we know, the variation could be driven by a single outlier, meaning perhaps only one omnivore’s labeled TMAO increased and that of the others remained flat. Or, perhaps it represents a large difference between the male and female subjects. With this level of variation, it seems unlikely that there was a statistically significant increase in TMAO among the omnivores at any specific time point, and the authors give no indication that this was so. When they compared the area under each curve, however, the difference was statistically significant.
While this may indicate that meat-eaters as a group generate more TMAO from supplemental carnitine than vegetarians, it is somewhat unclear whether this experiment was confounded by antibiotic treatment, and the authors do not explain whether the result is driven by a single outlier or a fundamental gender difference, neither do they show any results indicating that the total amount of TMAO in the blood (instead of just isotopically labeled TMAO) increased.
Do Omnivores Have Higher TMAO Than Vegetarians and Vegans Because of Meat-Induced Changes in Intestinal Bacteria?
Among 23 vegans and vegetarians and 30 omnivores, the authors reported differences in intestinal bacteria that they tied to blood levels of TMAO in the absence of a steak or carnitine challenge. The most dramatic difference seen was a roughly three-fold greater level of TMAO in the blood of four subjects with “enterotype 2,” with bacterial DNA from Prevotella species dominating their feces, when compared to 49 subjects with “enterotype 1,” with bacterial DNA from Bacteroides species dominating their feces. As the authors note in the discussion, enterotype 2 had previously been associated with “low animal-fat and protein consumption,” but three out of four subjects with this enterotype in the current study were omnivores.
Although the largest difference was seen between those with enterotypes 1 and 2, TMAO levels were nevertheless 45 percent higher among the meat-eaters than among the vegans and vegetarians. There were also significant differences in specific strains of intestinal bacteria between the dietary groups that could hypothetically account for this difference.
While it is possible that intestinal flora accounts for the difference, it is disappointing that the authors did not consider other possibilities, such as differences in the activity of the enzyme that converts trimethylamine to TMAO. For example, vitamin B2 is the main cofactor for the enzyme, and vegans are three times as likely to be deficient in vitamin B2 as vegetarians and omnivores.
To support their hypothesis that the difference in intestinal bacterial metabolism of carnitine can be induced by meat consumption, the investigators fed mice 1.3 percent carnitine in drinking water and showed that this altered intestinal flora and led to a ten-fold increase in the TMAO yield in response to a force-fed carnitine challenge. Before we take this as supporting evidence that people who eat meat have higher TMAO than vegans and vegetarians because of meat-induced changes in intestinal flora, we should consider a couple of caveats.
Suppose each mouse drinks about 5 milliliters of water per day. This would provide 65 milligrams of carnitine per day, more than a third of what could be obtained from eating an eight-ounce steak. Adjusting for body weight, this is like a human eating a thousand steaks per day. This is beyond the capacity of even the most die-hard meat-lovers.
Moreover, the bacterial species that showed up in greater concentrations in carnitine-fed mice and correlated with TMAO levels had no correspondence to those found in meat-eating humans. The authors put it this way:
Notably, a direct comparison of taxa associated with plasma TMAO concentrations in humans versus in mice failed to identify common taxa. These results are consistent with prior reports that microbes identified from the distal gut of the mouse represent genera that are typically not detected in humans.
For both of these reasons, the carnitine-fed mice provide little in the way of justification for viewing the differences in intestinal flora between vegetarians and omnivores as a result of consumption or abstention from meat.
While antibiotics wipe out TMAO levels in humans and mice, showing that intestinal bacteria are necessary for its formation, the authors provide no clear evidence that the specific differences in intestinal bacteria between vegetarians and vegans on the one hand and meat-eaters on the other cause the observed difference in TMAO levels.
It is unclear whether the 45 percent higher TMAO levels in meat-eaters represents something that we should regard as “unhealthy.” As I pointed out above, for all we know it could be due to riboflavin (vitamin B2) deficiency among the vegans. If we suppose for the sake of argument, however, that it does represent something unhealthy, there is no reason to connect it to the consumption of meat. As Chris Kresser pointed out in his critique of the Nature Medicine paper, most comparisons between vegetarians and omnivores are confounded by substantial lifestyle differences between these two groups. They are also confounded by dietary differences that have nothing to do with meat, such as the consumption of fruits and vegetables. While the possibility that long-term meat-eating itself increases TMAO levels remains a legitimate hypothesis to be investigated, equal investigation should be given to alternative hypotheses focusing on other dietary and lifestyle factors that differ between vegetarians and omnivores.
Does TMAO Cause Heart Disease?
Female C56BL/6J mice genetically engineered to be missing ApoE, an important protein involved in lipoprotein metabolism, developed twice as much atherosclerosis when fed a thousand steaks a day worth of carnitine. This and supplementary studies feeding mice TMAO suggested that TMAO derived from dietary carnitine may suppress the removal of cholesterol from the immune cells that populate atherosclerotic plaques. As proof of principle, these studies may have some value, but their relevance is questionable. Such an exorbitant amount of carnitine is surely irrelevant to human meat intake. The mice, moreover, are among the most vulnerable. They presumably used females because males convert trimethylamine to TMAO at a lower rate. ApoE knockout mice not only lack a critical protein that humans have, but the C56BL/6J background strain of mice, as I’ve written about before, has a deletion in a gene related to B vitamin and glutathione metabolism that prevents the mice from recycling glutathione in the presence of oxidative stress.
Can such a result be observed in male mice, in mice without these genetic defects, and in mice fed attainable quantities of carnitine? Without knowing the answers even to these preliminary questions, it seems unreasonable to consider these experiments relevant to human health at this stage of the game.
The authors also investigated the relationship between plasma carnitine levels and heart disease in just under 2600 humans undergoing elective cardiac evaluation. Males had higher carnitine levels than females. In the lowest quartile of carnitine status, only 54 percent of subjects were male. In the highest quartile, 80 percent were male. Those who had the highest carnitine levels were more likely to smoke (77 percent) than those who had the lowest (61 percent). The majority of the subjects were on ACE inhibitors, beta-blockers, statins, and aspirin. Those with higher carnitine levels had a greater likelihood of having cardiovascular disease, peripheral artery disease, and cardiovascular disease. Statistical adjustment for traditional cardiovascular risk factors attenuated the associations. We can imagine that if it were possible to identify all of the confounding factors, further statistical adjustment would further reduce and perhaps eliminate the association.
The authors provide no evidence that the variation of plasma carnitine in these subjects primarily reflects variations in dietary carnitine intake, and there is no particular reason to assume this. To offer one counter-example, in guinea pigs, one of the few experimental animals that have a dietary vitamin C requirement like humans do, vitamin C deficiency leads to a loss of carnitine from muscle and an increase in plasma carnitine. Vitamin C probably protects against heart disease by preventing lipoprotein oxidation in the blood and by promoting collagen synthesis in arterial plaques, which protects them from rupture. Perhaps plasma carnitine is an inverse marker of vitamin C status.
In a separate analysis, blood levels of carnitine appeared to associate with cardiovascular events only in the presence of high blood levels of TMAO. This is consistent with the authors’ hypothesis that carnitine contributes to cardiovascular disease through its conversion to TMAO, but it could be consistent with a number of other hypotheses as well. Perhaps blood levels of TMAO reflect intestinal dysbiosis, variations in the activity of the enzyme that converts trimethylamine to TMAO (as I wrote in my last post on this topic, activity of the enzyme could reflect drug exposure, genetically determined drug efficacy, iron overload, ethnicity, or other factors), or perhaps TMAO increases in heart disease to play important physiological roles such as protein stabilization.
This study provides a foundation for future studies to investigate whether TMAO can be used as an independent predictor of heart disease risk and whether TMAO and carnitine status can be used as markers of clinically relevant metabolic changes, but it hardly provides us with a basis for believing that carnitine from fewer than a thousand steaks per day causes heart disease through its conversion to TMAO.
The Bottom Line
The bottom line here is that the popular interpretation of this study as an indictment of red meat makes no sense. Even if physiological levels of TMAO contribute to heart disease in humans (which is a big “if” at this point) and even if red meat were to raise TMAO substantially more than most other foods (which appears to be false), it wouldn’t in any way whatsoever follow that eating red meat causes heart disease. The biological effects of a food cannot possibly be reduced to one of the biological effects of one of the food’s components. Believing such a thing would require believing not only that the particular component has no other relevant biological effects, but that there are no relevant biological effects of any of the other tens of thousands of components of that food.
As Chris Kresser pointed out today, the balance of epidemiological evidence fails to show an association between fresh, unprocessed red meat and heart disease. Numerous studies, including randomized trials, have suggested that carnitine supplementation improves outcomes in patients with cardiovascular disease. Carnitine thus may be a generally heart-protective nutrient. The authors acknowledge these studies in their discussion but suggest that carnitine may have conflicting effects, especially when used orally rather than intravenously as in some studies, since the oral route allows exposure to intestinal bacteria.
If the carnitine in red meat were promoting atherosclerosis through its conversion to TMAO, however, then red meat should be no more dangerous than potatoes and carrots and the real killer should be seafood. How likely is this to be true? Prospective studies correlate fish consumption with a reduced risk of heart disease mortality. Some Pacific Island groups that eat seafood regularly, such as the Kitavans, appear to be free of heart disease. Randomized trials have tended to focus on fish oils rather than whole fish. Those testing advice to eat more fish are ambivalent, but they don’t seem to suggest that eating whole fish increases the risk of heart disease.
The elucidation of nutritional pathways and biochemistry in this paper is interesting, but it shouldn’t serve as a reason to avoid red meat.
Read more about the author, Chris Masterjohn, here.
Acknowledgments
Thanks to Chris Kresser, Stephan Guyenet, Ned Kock, and Peter Attia for discussing some of the points made in this post.
Notes
* Of course it would be better if we could see these foods and the control breakfast compared to a control of pure water or something that should be similarly ineffective at generating TMAO. A certain proportion of the TMAO excreted in the urine could perhaps be due to endogenous trimethylamine precursors circulated through the gastrointestinal tract. Nevertheless, this should be similar across foods. Additionally, the authors did not specify the mix of foods in the “light breakfast.” Thus, it is unclear how much TMAO for each item comes from the light breakfast and how much from the food being tested. The only certain thing is that those foods yielding statistically greater TMAO excretion generated more TMAO than the control and the other foods tested.
** One-way ANOVA using Dunnet’s post-test to compare all values to beef and adjust for multiple comparisons, using Graphpad Prism 5.
*** Did these subjects generate substantially less TMAO from red meat than the subjects in the new Nature Medicine paper? It would seem not. The Nature Medicine paper reports urinary TMAO excretion in different units, and it reports TMAO alone rather than the sum of it and its precursor, trimethylamine. Nevertheless, according to my calculations, the “representative female omnivore” excreted a little under 212 micromoles/8 hours, whereas the average excretion after eight ounces of beef in the 1999 study was 76.5 micromoles/8 hours, indicating perhaps slightly higher but more or less similar generation of TMAO after red meat between the studies, especially considering the variation in responses in the 1999 study (SD 48.5) and compared to seafood. The modestly larger amount reported in the Nature Medicine could easily be explained by the extra 250 milligrams of supplemental carnitine provided, and perhaps by the use of TMA + TMAO rather than TMAO alone.
Assuming the average person clears about 1 mg creatinine into their urine per minute (480 mg/min) and 113.12 g/mol creatinine (thus 480 mg/1000 mg/g and divided by the molar mass, multipled by 1000 to convert mol to mmol, yielding an average excretion of 4.24 mmol creatinine in 8 hours), I calculate that just under 50 mmol TMAO/mol creatinine, as shown in Fig 2b of the Nature Medicine paper converts to 212 umol/8 h (50 mmol TMAO/mol creatinine * 1 mol creatinine/1000 mmol creatinine *4.24 mmol creatinine/8 hours * 1000 umol/TMAO/mol TMAO).
Christopher Masterjohn